


Blood Tests, Cholesterol, Saturated Fats, and Heart Disease: The Facts

The lipid hypothesis claimed a connection between saturated fat, cholesterol, and heart disease. The first postulate of this theory is that a diet high in saturated fats raises blood cholesterol, and the second postulate is that this high cholesterol level drives the development of heart disease or atherosclerosis.
A Brief History of the Lipid Hypothesis
The very foundations of the lipid hypothesis were built on bias by its founder, Ancel Keys. He observed that there is cholesterol in coronary artery plaque and that animal foods contain cholesterol, so he stated that animal foods must cause this plaque.
The logic behind this simplistic conclusion is seriously flawed, as the same argument could be made that fire trucks cause fires because fire trucks contain firemen, and firemen are always found where there’s a fire.
Ancel Keys published the “Seven Countries Study,” in which he interviewed 12,700 middle-aged men in several countries and measured health outcomes. His published results were said to prove the lipid hypothesis, laying the cornerstone of one of the biggest healthcare failures of the century.
In a stunning example of confirmation bias, Ancel Keys omitted countries whose data did not match his hypothesis. As reported by Nina Teicholz in her book, The Big Fat Surprise, France, Switzerland, and Chile were omitted as they had high fat consumption but low instances of heart disease. There is no statistical significance whatsoever when all twenty-two studied countries are included.
What Is Cholesterol?
Cholesterol, a waxy and fatty substance produced in the liver and the intestines, is essential for the integrity of cell membranes and the production of vitamin D and hormones. Cholesterol is also absorbed from food.
Whether or not cholesterol causes atherosclerosis is hotly debated. What is becoming clear, though, is that there are different types and sizes of cholesterol particles, some of which seem more harmful than others, depending on their size and quantity in the blood.
Lipids are not water-soluble, so to move through the bloodstream, they are attached to water-soluble proteins, hence the name lipoprotein.
Heart Disease in America
Cardiovascular disease is a leading cause of death among U.S. adults. Between 2015 and 2018, 126.9 million US adults had some form of cardiovascular disease, a huge “F” for the success of care plans based on the lipid hypothesis in preventing cardiovascular disease.
An August 2020 research paper in the Journal of the American College of Cardiology pointed out that trials of reducing saturated fat did not show a meaningful reduction in heart disease, though reducing carbohydrates and insulin resistance lessens heart disease risk. This isn’t a startling amount of support for a concept so widely accepted.
When citing positive outcomes for statin use, “relative risk” is often enlisted. As an example, a recent paper highlighted the use of relative risk rather than absolute risk. The researchers evaluated 21 trials and found that the absolute benefit of statin therapy was negligible at best. These papers claimed a risk reduction of up to 29% for statin therapy, but that represented less than 2% absolute risk reduction.
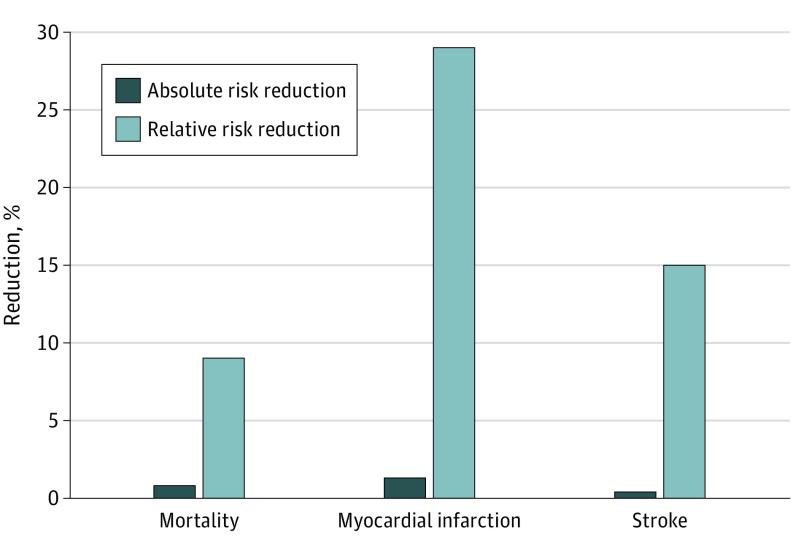
What is relative risk reduction? Here’s an analogy to help illustrate: Would you accept a person's offer to double your chances of winning the lottery? You'd get a second lottery ticket and have twice the chance of winning. But that's two in a billion instead of one in a billion, which isn't a big enough difference to get excited about, is it?
Understanding Blood Tests
Blood testing can be a valuable tool to identify problems and validate dietary outcomes. It is also a frequent talking point with individuals following a low-carb diet, as some of the values can raise eyebrows from practitioners unfamiliar with this health strategy.
Let’s review some of the most common lipid tests and provide some science-based interpretations that are more consistent with current knowledge when compared to commonly held beliefs.
We will also review some of the newer tests and evaluation ratios that have been validated and are beginning to get traction in the functional care community. This is for your information, but always have your provider review your lab results with you.
Cholesterol
Immune function Circulating lipoproteins that contain cholesterol serve a vital role in immune function. An article published in the October 1998 journal Epidemiology & Infection showed that elevated levels of lipoproteins are protective against Salmonella infection, for example.
Total cholesterol was found to be inversely related to infections requiring hospitalization, meaning that elevated cholesterol is probably protective in nature.
Is elevated cholesterol dangerous? While it is a commonly held belief that elevated cholesterol, particularly LDL lipoprotein-bound cholesterol, is dangerous, that hypothesis is not entirely supported by the research. It is important to confront this fact directly and understand it because adopting a diet with no processed foods and more animal-based protein may cause cholesterol values to rise in some people.
Well-meaning family members and healthcare workers often suggest a change in diet and statin medications. But what if elevated cholesterol was associated with longevity? There is evidence that lower cholesterol values are associated with increased all-cause mortality, suggesting cholesterol has a protective value. First, let’s take a closer look at cholesterol numbers.
Types of Cholesterol and Implications
The following briefly explains the different forms of cholesterol and how they act in the body.
Total cholesterol This number represents the sum of your HDL, LDL, and VLDL cholesterol numbers. If the math “doesn’t add up” and the sum of these is less than your total cholesterol, the difference is known as “remnant cholesterol.” While many people may believe that keeping this number “under 200” or even less would be beneficial, that’s not necessarily what the data show.
A study looked at total cholesterol levels and all-cause mortality (your chances of dying, from anything) and concluded that low cholesterol was much more dangerous than elevated cholesterol. The total cholesterol level with zero additional risk was 250, with only a slight increase noted at 300. Any increase in mortality from elevated cholesterol was greatly reduced by age. The graph below shows these associations for different age groups in the study.
.jpg)
(Yi SW, Yi JJ, Ohrr H. Total cholesterol and all-cause mortality by sex and age: a prospective cohort study among 12.8 million adults. Sci Rep. 2019 Feb 7)
HDL cholesterol HDL picks up cholesterol in the blood and takes it to the liver for removal. This has been hailed as “the good cholesterol” for quite some time, and current opinions still reflect that esteemed status. A higher HDL level is associated with a reduced risk of heart disease or mortality.
LDL cholesterol This lipoprotein has been the “cardiac villain” for decades, yet there is significant evidence that the story isn’t quite so simple. Our immune system depends on LDL cholesterol, and studies of people with very high cholesterol levels due to their genetics (familial hypercholesterolemia or FH) have shown that when untreated for their elevated cholesterol these people live longer lives and have no meaningful increase in heart disease compared to individuals with “normal” LDL levels.
A more up-to-date point of view is that cardiovascular disease is caused by inflammation and not by cholesterol, and focusing on diet, exercise, and healthy lifestyle choices is more likely to reduce heart disease risk.
VLDL cholesterol This designation is very-low-density lipoproteins, and they have been found to promote cardiovascular disease in people with type 2 diabetes. VLDL moves mostly triglycerides through the blood to fat and muscle tissue, where it is broken down and eventually metabolized into LDL, or low-density lipoprotein. There are two types of LDL: large and small.
Large low-density lipoprotein is lighter and less easily attached to artery walls than small LDL. A diet high in saturated fats tends to boost this number.
Small low-density lipoprotein is denser than large LDL and can more easily stick to artery walls than large LDL, where it oxidizes and inflames the wall of the artery. Factors like smoking or high blood pressure can also cause inflammation and damage to the walls of the arteries.
The inflammation activates the immune system, which then begins to patch the artery walls, resulting in plaque buildup. These lipoproteins are largely increased by eating a low-fat, carbohydrate-rich diet.
Triglycerides
All carbohydrates consumed, whether sugar or starches, break down into glucose during digestion. Some carbohydrates are burned as fuel; anything left is stored in the liver or fat cells. When the liver cannot store more glucose as glycogen, extra glucose is stored in fat cells. When fat cells can no longer store more fatty acids and release them into the bloodstream, triglyceride levels in the blood will rise.
Triglycerides are fats that are transported in the bloodstream. The name is an abbreviation of triacylglycerol, a form of fatty acid and glycerol ester that allows it to flow through the blood. Elevated triglycerides are considered a risk marker for heart disease as well as a marker of inflammation. The ratios of blood values are also sometimes very accurate predictors of cardiovascular risk.
Elevated triglycerides are considered a marker for the probability of heart disease and cardiovascular disease risk by directly contributing to cholesterol deposition in the arterial wall as well as activating inflammatory, apoptotic, and clotting pathways.
Carbohydrates, Insulin, and Triglycerides The consumption of high levels of dietary carbohydrates results in elevated insulin levels, as insulin must be produced to store the excess blood glucose in fat cells. The fat cells eventually become insulin resistant, causing fatty acids to remain in the bloodstream. This mechanism drives elevated blood triglyceride levels when too many carbohydrates are consumed and is one of the core mechanisms in the development of atherosclerosis.
Triglyceride: HDL ratio Dividing the level of triglycerides by the level of HDL cholesterol can provide a numerical risk assessment. The triglyceride : HDL ratio can predict atherosclerotic risk and the probability of heart disease. A lower ratio predicts a lower cardiac risk, with below 1.0 being very desirable. A level over 3.0 is considered to indicate a significant risk of heart attack or stroke, and this increases proportionally with higher ratios. To calculate this ratio, divide the triglyceride number by the HDL cholesterol number.
Triglyceride-Glucose index This index consists of the log of the triglyceride level multiplied by the glucose level and has been validated as a very reliable indicator of insulin resistance and all-cause or cardiac mortality. It is generally calculated by using one of the online calculators and submitting the glucose and triglyceride values into the suggested fields.
Inflammation
Inflammation is also a key factor that results from elevated triglyceride levels and affects endothelial function in the blood vessels. The sustained inflammatory process contributes to insulin resistance. This combination promotes atherosclerotic heart disease.
One of the primary methods of injury to the heart’s blood supply is inflammation. When that occurs, the body attempts to heal the resulting damage. Small, dense LDL particles become adhered to the lesion, where they can become damaged through a process known as oxidation.
hs-CRP High sensitivity C-reactive protein is a marker of inflammation, particularly of the blood vessels. When this is elevated, it indicates that the body is in an inflamed state. While an elevated CRP level does not explain the cause of the inflammation, it is a reliable marker for chronic inflammation due to many causes, such as infection or food reactions.
Homocysteine This marker is an amino acid produced when methionine donates a methyl group during methylation reactions involved in detoxification and DNA maintenance. It can normally be re-methylated using the enzyme methylenetetrahydrofolate reductase (MTHFR) or converted to cysteine. Homocysteine is inflammatory to the blood vessels and can promote atherosclerosis.
When there is a genetic defect in the MTHFR gene (C677T or A2398C), the process does not work as efficiently, and homocysteine may accumulate. This can also result in a deficiency of methionine, as homocysteine isn’t converted back to methionine efficiently.
A homozygous mutation can result in a 60% reduction in this conversion rate, while a heterozygous mutation may only reduce it by 30% or less. Of note is that eggs and meat can provide choline, and increasing choline intake can support methylation and compensate for the MTHFR variant genotype.
Other causes of increased homocysteine include folate deficiencies (MTHFR converts folate to methyl folate, a bioactive form), vitamin B6, or vitamin B12.
Apolipoprotein B ApoB is a cholesterol-carrying lipoprotein increasingly regarded as having a significant role in causing atherosclerosis. ApoB is made of chylomicrons, VLDL, LDL, and lipoproteins. These molecules can penetrate the endothelial cells lining the arteries and cause damage, initiating the cascade of inflammatory events that result in foam cells, oxidized LDL, and consequent plaque formation. It has also been shown that ApoB, which is high in triglycerides and known as remnant lipoproteins, is the most dangerous.
The Role of Oxidized LDL Oxidized LDL (particularly LDL with high levels of apolipoprotein B, which are small, dense LDL) at the site of an endothelial lesion results in further inflammatory changes, which then recruit white blood cells to help heal the damaged endothelium.
These immune cells phagocytize (engulf and try to destroy) the oxidized LDL particles in an attempt to clean up the cellular debris. As they get bloated with all of the LDL particles they have consumed, their physical form changes to foam cells. This is the beginning of a “fatty streak," an atherosclerotic lesion.
Coronary Artery Calcium Score
A coronary artery calcium (CAC) score isn’t a lab test but a short CT scan of the heart, which demonstrates the extent of calcification in the coronary arteries. This is an excellent test to evaluate the risk of a major heart attack, even in an individual otherwise considered low risk and having no symptoms. The degree of calcification is assigned a score, with zero indicating no calcification at all.
The logic behind the test is that if the calcification is present in the coronary arteries, an individual might still be asymptomatic and perform normally on an exercise tolerance test, yet be at risk of a calcified plaque flaking off and initiating a massive clotting event and heart attack.
This test takes only a few minutes and is not expensive compared to other forms of testing.
Start making real progress

Related

Importance of a Low-Carb Diet for Treating Metabolic Conditions

How Revero Treats Autoimmune and Inflammatory Conditions
